Personal is Political: On Institutional Abuse in Psychiatric Facilities (Part II)
By Guojun Susana Lee
Fear and dissociation dominated the environment. Above the dispensary window was a stenciled quote underlined with red hearts: “There is no time in my life to be sad or mad.” The staff’s insensitive actions reinforced this statement. Once, in the middle of the lunch line, a social worker asked me why I cut myself and whether it was for attention. I felt deeply violated. Even so, I thought that I could reach out to him by being honest about myself, however difficult. I had barely begun, however, before he uttered, “That’s enough” and walked away. He was the same social worker who, after my discharge, told me to take a cab straight to my dorm so that no one would know what I had done or where I had been.
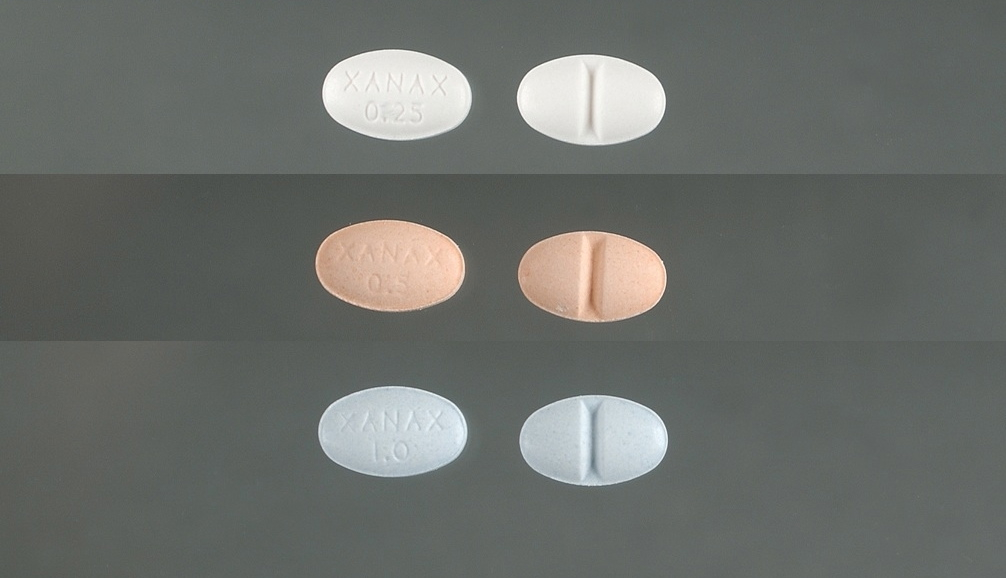 I only realized the chilling extent to which that quote described the facility when I first talked to Lena as she sat on the floor before the dispensary window waiting for her meds, so jittery from withdrawal that she wanted to “tear out her skin.” Benzos—proven harmful and addictive—are a common category of drugs administered to patients. I listened to my friends talk about horrifying side effects. Asked by a scared patient if any medication existed without side effects, a nurse dismissed the question. “No. Even the air we breathe can be over-oxygenated.”
I only realized the chilling extent to which that quote described the facility when I first talked to Lena as she sat on the floor before the dispensary window waiting for her meds, so jittery from withdrawal that she wanted to “tear out her skin.” Benzos—proven harmful and addictive—are a common category of drugs administered to patients. I listened to my friends talk about horrifying side effects. Asked by a scared patient if any medication existed without side effects, a nurse dismissed the question. “No. Even the air we breathe can be over-oxygenated.”
Unfortunately, some patients would adopt similar tactics, especially by mocking other patients. Once, a nurse sat in the day room gossiping to us about manic and schizophrenic patients in a “lower-functioning” unit. She managed to convince patients from our unit to ridicule the patients in Unit 400. How they urinate in the couches. How a woman tried to take her clothes off during a smoke break. How another woman poured water down the hallway and declared that her water had broken. How all the women think they are pregnant. There is no consideration for the patients’ suffering. As a result, the nurse deprives all the patients in Unit 400 of their mattresses and smoke breaks if even one individual misses a group session. When I spoke out against the abuse, along with the violations I had experienced and witnessed in our unit, she responded by telling me that “some of the patients had come willingly.” I responded that this was no justification for any form of disrespect. After this exchange, many of the patients told me in private how much they agreed with me. At the time, however, Lena tried to play the role of peacekeeper by offering that I simply needed to “wake up to the reality of psychiatric facilities.” Similarly, many patients in our unit agreed from experience that this facility was “the best there was” in comparison to others in the area. They had been through far worse. This alone illustrates the fact that institutional abuse becomes patients’ normalized reality.
This is possible because the facility made it difficult for us to process our experiences in the context of the wider world or to visualize ourselves in that context, which is necessary for psychological healing. Conversely, treatment at this facility included cutting a patient off from life outside of it. During my cold, sleepless night, I was only able to convince the staff to give me, albeit begrudgingly, a short, blunt pencil and a single sheet of paper for writing. Convincing the employees to let me have my book, which sat by the glass window purportedly awaiting inventory, took many times more effort.
This results in profound isolation with tremendous consequences. In the room where patients are told to strip, I was allowed only a five-minute phone call without privacy before my cell phone was taken from me. Patients are only allowed to use the unit’s two phones in the absence of scheduled activities, which take most of the day. These phones are located in the day room and hallway, and any long-distance call has to be accomplished before 10 pm, and requires a nurse to dial the number from one of their phones. This prevents patients from sharing their doubts and grievances with the outside world, and it cuts off patients’ access to reminders that their treatment is neither normal nor healthy.
 When I was finally discharged, I reminded a nurse that they were still holding on to my boots and a bag containing my valuables. I could easily have missed this and was worried about the patients who are too sick or medicated to make sure their belongings are returned. I still worry about this. In order to look behind the desk, the nurse put me back under lock and key, because I could not be left “unsupervised.” When she returned, she spoke to me in a voice you would likely only hear people use to speak to infants, “Ready to try again?” On the way out, I ran into the other patients headed to dinner. We hugged. One of them called out to wish me well and was told by employees to “hush.”
When I was finally discharged, I reminded a nurse that they were still holding on to my boots and a bag containing my valuables. I could easily have missed this and was worried about the patients who are too sick or medicated to make sure their belongings are returned. I still worry about this. In order to look behind the desk, the nurse put me back under lock and key, because I could not be left “unsupervised.” When she returned, she spoke to me in a voice you would likely only hear people use to speak to infants, “Ready to try again?” On the way out, I ran into the other patients headed to dinner. We hugged. One of them called out to wish me well and was told by employees to “hush.”
This particular facility may not leave any marks on our skin, but the scars it leaves are still profound. I fell into a more severe depression than I had ever experienced and considered dropping out of college, because my institutionalization triggered traumatic memories: being trapped in circumstances against my will and having the things that mean the most to me invalidated or taken. A major part of the depression also came from the negative messages about myself that lingered from being locked-up, policed, ignored, avoided, and feared. But it was mainly the continuing sense of overwhelming isolation. The feeling that no one will ever understand the nightmares. That the facility would simply cover up any mistreatment if an investigation should occur. That everyone else, in their well-meaning effort to help frame my experience at the hospital in a positive light, has failed to grasp the mistreatment still happening to the friends I left behind. It has been weeks since my discharge and I am not yet able to put on the clothes I wore to the facility or eat animal crackers. Fire alarms around my college campus remind me of the facility, because I had gone through every possible means of escape, including setting off the alarms and making a run for it.
Without the empathetic bond among patients in the unit, I might not have pulled through. We worked together to ensure that Justine, another patient, always had an extra chair for her injured leg. We invited elderly patients to step ahead of us in the lunch line, even if they were from a different unit. Lena once talked a young girl out of taking her life in an adolescent unit by sharing the story of her sister’s suicide.
 In the middle of a recreational therapy session, while a guitarist was playing, Agnes and Sarah decided spontaneously to jump up and dance. I ran over to join them. Tracie followed. We danced in a circle and it was the most dignifying moment in my entire time at the facility. During the same session, Tracie was moved to sing a snippet of a song with the guitarist and the entire gymnasium began singing along. Her voice was truly beautiful. All the way back to the unit, she told Sarah and I about how she used to sing, brightened and anchored by the memories. Shortly after, however, Tracie came to us on the other side of the glass screen, visibly disturbed by the effects of her medication. “I have forgotten the lyrics to this song…I used to sing it acapella.”
In the middle of a recreational therapy session, while a guitarist was playing, Agnes and Sarah decided spontaneously to jump up and dance. I ran over to join them. Tracie followed. We danced in a circle and it was the most dignifying moment in my entire time at the facility. During the same session, Tracie was moved to sing a snippet of a song with the guitarist and the entire gymnasium began singing along. Her voice was truly beautiful. All the way back to the unit, she told Sarah and I about how she used to sing, brightened and anchored by the memories. Shortly after, however, Tracie came to us on the other side of the glass screen, visibly disturbed by the effects of her medication. “I have forgotten the lyrics to this song…I used to sing it acapella.”
I made a commitment then and there to do everything within my power to make mental healthcare a safe and affirming space for all the songs in a patient’s heart. But this work belongs to all of our communities. Many of you are already doing this work. You may even have made this your life’s work. My appreciation goes out to you for your work. At this time, I am in the process of opening up media channels to bring together patients, health professionals, journalists, and civil rights activists to facilitate dialogue and investigations. I hope you will join me by sharing my story and, maybe, your own. Please visit the Remembering our Songs website and Facebook page to share your story and learn more about how you can make a difference.
NOTE: Read Part I of “On Institutional Abuse in Psychiatric Facilities” here.
 Guojun Susana Lee recently graduated from Colorado College with a degree in Critical Regional Studies and Psychoanalysis. She is proud to call northern New Mexico her home, and she continues to be involved in grassroots movements surrounding cultural literacy, social and environmental justice, and Indigenous medicine in the area. She is part of the Indigenous Alliance without Borders, based in Tucson, AZ. Singing, long redeeming walks, chile over runny yolk, poetry, and synesthesia are indispensable to her world. Guojun is in the middle of writing her first novel, Proof of Residence, and she dreams of becoming a midwife.
Guojun Susana Lee recently graduated from Colorado College with a degree in Critical Regional Studies and Psychoanalysis. She is proud to call northern New Mexico her home, and she continues to be involved in grassroots movements surrounding cultural literacy, social and environmental justice, and Indigenous medicine in the area. She is part of the Indigenous Alliance without Borders, based in Tucson, AZ. Singing, long redeeming walks, chile over runny yolk, poetry, and synesthesia are indispensable to her world. Guojun is in the middle of writing her first novel, Proof of Residence, and she dreams of becoming a midwife.



Pingback: On Institutional Abuse in Psychiatric Facilities | The Feminist Wire